How Often Should Privacy Awareness Training Be Provided
What Is the Best Practice for Privacy Awareness Training?
Privacy awareness training should not be a one-time event. Best practice is to provide privacy awareness training annually and reinforce key concepts throughout the year.
This expectation is frequently reinforced by privacy regulators, including the Office of the Information and Privacy Commissioner (OIPC), in privacy breach investigation reports. Organizations are expected to demonstrate that privacy awareness is an ongoing program rather than a single training activity.
As a best practice, I recommend that all employees complete comprehensive privacy awareness training at least annually, supplemented by ongoing refresher activities throughout the year. Annual training helps reinforce foundational concepts, demonstrate accountability, and ensure your organization can show consistent compliance if it is ever reviewed.
Most Privacy Breaches are Caused by People, Not Technology
Privacy training is often treated as:
- A checkbox
- A one-time event
- Something to “get done”
However, most privacy breaches are caused by people, not technology. Common examples include:
- Curiosity snooping
- Misdirected communication
- Lack of awareness
- Inconsistent practices
- Failure to follow established procedures
Technology plays an important role in protecting information, but employees make decisions every day about how information is collected, used, disclosed, and safeguarded. Effective privacy awareness training helps employees make the right decisions when faced with real-world situations.
Privacy awareness training is one of the most effective ways to prevent avoidable privacy breaches.
Privacy Awareness Training Is Your First Line of Defense
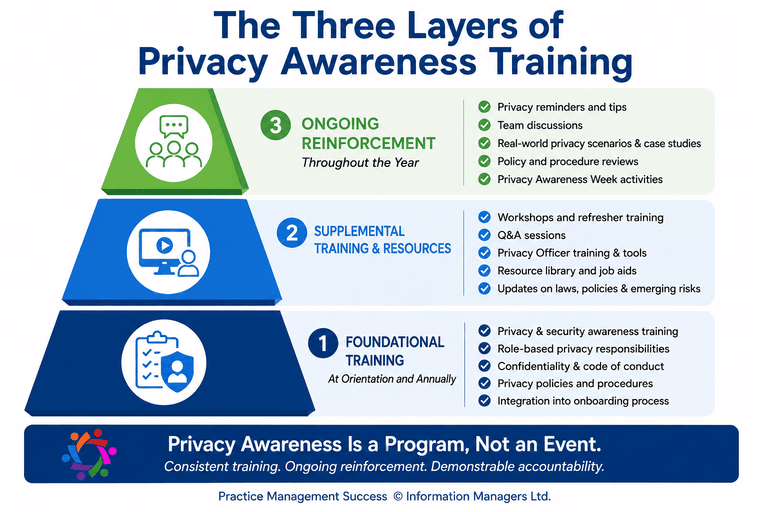
To make privacy awareness training practical and effective, think of it as a program with three layers:
1. Foundational Training (At Orientation and Annually)
Provide comprehensive privacy and security awareness training to all employees, vendors, and business associates at onboarding. The Corridor Interactive Healthcare Essentials course is an easy-to-implement solution that supports consistent training across the organization:
Privacy awareness training should then be repeated annually for all staff. Alternate the annual content with the Corridor Refresher Privacy Awareness Training (PAT) and with supplemental training and resources to keep content engaging, relevant and current.
2. Supplemental Training and Resources
Annual training provides the foundation, but employees benefit from additional learning opportunities throughout the year. Information Managers’ Practical Privacy Officer Strategies training includes a module on designing and implementing a privacy awareness training plan that you can reuse year after year. This on-line course is ideal for privacy officers and clinic managers.
Practice Management Success membership includes monthly Q&A sessions and practical training topics you can use for refresher training throughout the year. Workshop-on-demand topics include privacy breach management, release of information best practices, AI Governance, and more!
3. Ongoing Reinforcement (Throughout the Year)
The most effective privacy programs keep privacy visible throughout the year.
Reinforce key concepts through:
- Short privacy reminders
- Team discussions
- Privacy breach case studies
- Staff meetings
- Policy and procedure reviews
- Privacy Awareness Week activities
Use real-world privacy scenarios and your organization’s policies and procedures as discussion tools to keep expectations clear and top of mind.
These small but consistent reminders help employees apply privacy principles in their day-to-day work and reduce the risk of privacy incidents.
What Regulators Expect: Demonstrable Accountability
Privacy awareness training is not simply a best practice—it is often a factor considered by privacy regulators when investigating privacy breaches.
For example, in Ontario PHIPA Administrative Monetary Penalty, a healthcare worker repeatedly accessed patient records without authorization. The Information and Privacy Commissioner emphasized the organization’s responsibility to implement safeguards, monitor compliance, and ensure employees understand their privacy obligations. While policies existed, the case highlights the importance of ongoing privacy awareness, monitoring, and reinforcement to prevent curiosity snooping and other inappropriate access.
Similarly, privacy commissioners across Canada frequently examine whether organizations can demonstrate that employees received privacy training and understood their responsibilities. During investigations, regulators often ask for evidence such as training records, attendance logs, signed confidentiality agreements, policy acknowledgements, privacy reminders, and documentation of corrective actions.
This is where many organizations struggle. They may have policies and procedures, but they cannot demonstrate that employees reviewed them, understood them, or applied them in practice.
When a privacy breach occurs, documentation matters. Organizations that can show a planned privacy awareness program, annual training, ongoing reminders, and documented participation are in a much stronger position to demonstrate due diligence and accountability.
The lesson is simple: privacy awareness training should not be viewed as a one-time event. It should be an ongoing program that helps employees recognize risks, make good decisions, and protect patient information every day.
Privacy regulators and group practice reviews increasingly focus on an organization’s ability to demonstrate accountability.
You must be able to demonstrate:
- Training is planned and intentional
- Staff participated in training
- Staff understood key concepts
- Training is relevant to employee roles
- Privacy awareness activities occur throughout the year
This concept is often referred to as demonstrable accountability.
Demonstrable accountability means having evidence that your privacy program is working—not simply having written policies and procedures sitting on a shelf.
See Why “Demonstrable Accountability” Matters
Need Help to Create Your Privacy Awareness Program?
In the Practical Privacy Officer Strategies training, you quickly create a privacy awareness plan that can be reused and updated each year.
A successful privacy awareness program combines annual comprehensive training with ongoing reinforcement throughout the year. This approach helps reduce privacy risks, supports employee confidence, and demonstrates the due diligence and accountability expected by regulators, patients, and healthcare organizations alike.